Over the past weeks, as state and country leaders have begun considering easing social and economic restrictions, testing – specifically, the capacity to perform an adequate number of tests to track the spread of infections - has emerged as one of the most important topics of discussion and debate.
Currently, most tests used are Polymerase Chain Reaction (PCR) tests. The PCR test diagnoses active infections through a sample – usually a nose swab – that is processed to extract genetic material, of which the PCR technique makes thousands of copies (“amplifies”) to identify traces of viral genetic material found in the sample. This enables treatment and isolation of currently infected persons, and the implementation of contact tracing to break the transmission chain.
However, to test whether a person has been infected by the virus in the past, antibody tests – also known as serological tests – are required. Since antibody tests indicate the proportion of the population that has already been infected (and who are theoretically immune to the virus), they have attracted increasing attention as governments around the world explore different strategies to reopen their economies.
Moreover, expanded antibody testing is critical to better understanding for example how deadly COVID-19 is, which is still unclear. While early estimates from Wuhan, China showed a fatality rate between 2 – 3.4%, and the WHO calculated a rate of 3.4%, revised rates from Wuhan, and a study using data from the Princess Diamond Cruise showed lower rates of 1.4% and 1.3%, respectively.
More recent results reported in Los Angeles, Santa Clara and New York City, leveraging not yet published results from antibody testing, show more people have already been infected than was previously believed. The implications of higher spread are that fatality rates could be as low as 0.5% (New York City) and 0.12% (Santa Clara). These findings may affect policy makers’ decisions about ongoing closures. However, experts have cautioned against basing decisions solely on the results of these antibody tests, as concerns have been raised regarding the sampling of the studies, and the margin of error of the antibody testing (which can deliver false positive rates above 50% in a context of low prevalence).
Some countries are significantly ahead of others when it comes to testing capacity. One measure of testing capacity is the positivity rate, which is the share of PCR tests performed that return a positive COVID-19 infection. For example, for two countries with the same number of confirmed cases, the country with the higher positivity rate would signal a larger population that is infected, but not yet been tested. Lower positivity rates signal that the country is doing more testing and thus doing better at identifying those infected.
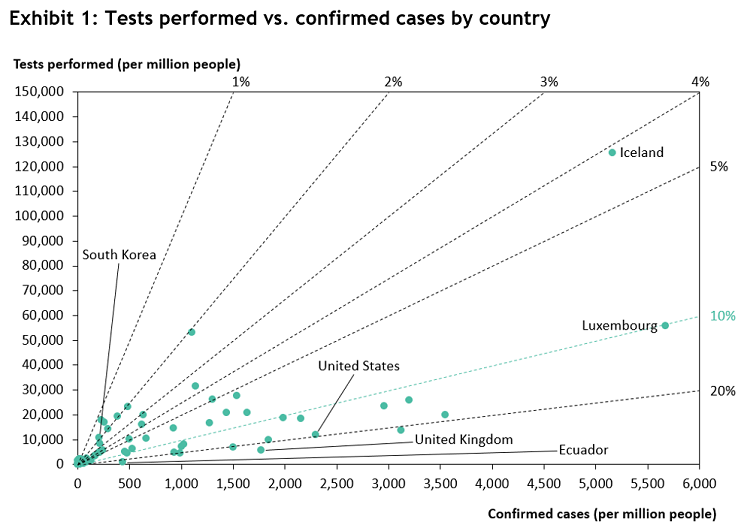
Exhibit 1 shows the total number of PCR tests performed and total number of confirmed cases per 1 million people for a range of countries. The dotted lines represent the respective positivity rates. Ecuador, which has the highest recorded positivity rate, saw 431 cumulative confirmed cases of COVID-19 and performed 901 tests as of April 15, giving it a positivity rate of 48%. The United Kingdom is also recording a high positivity rate of 31%, according to the most recent data. At the other end of the spectrum, Taiwan, South Korea, and New Zealand have been able to achieve positivity rates of 1 to 2%. As a benchmark for adequate testing, the WHO recommends that countries don’t exceed the maximum of 10% positivity rate - many of the larger countries, including the United States, have surpassed that maximum.
In the remainder of this newsletter, we highlight the roadblocks countries are facing in providing adequate testing and utilizing the results to inform crucial decisions.
Roadblocks to achieving adequate testing
- Shortage of testing supplies:
Materials required for PCR tests broadly consist of a swab that is used to collect patient samples, chemical reagents that isolate and process parts of the sample for analysis, and laboratory equipment that analyzes the processed samples. Country and state leaders are facing shortages for test kits broadly, but the largest bottleneck to creating an adequate test supply is proving to be the production of chemical reagents. A number of factors have led to the current shortage: first, during times of normalcy countries typically do not stockpile reagents, leading to a lower baseline level of supply; second, the global nature of the pandemic (as opposed to more targeted epidemics that only affected specific countries) have led to all countries demanding the same reagents at the exact same time, and; third, production of reagents has historically been concentrated in certain parts of the world.
Whilst this issue has impacted governments in almost all parts of the world, poorer communities with no native manufacturing capacity are disproportionately affected: countries in Africa and South America have reported waiting times of months for orders of testing kits. Even in the United States, shortages of swabs, reagents and chemicals required for PCR tests have also been a threat to increasing test capacity. In South Korea, by contrast, the government has been stockpiling the necessary chemicals for years after COVID-19’s cousin MERS briefly hit the country in 2015, which together with an early drafting in of the private sector to develop tests (when there were as few as four known cases in the country), helped the country move quickly.
- Poor quality of test kits:
In addition to supply shortages, errors in laboratory procedures and test development, as well as lack of expertise in commercial manufacturing have led to significant quality issues. For example, the US CDC’s initial batch of COVID-19 PCR detection tests showed faulty results and ultimately had to be recalled. Quality concerns have now also been raised in the US about the companies allowed to sell antibody test kits (the majority of which come from China), with some kits showing reliability levels as low as 20%. Germany, leveraging its position as leader in lab technology, is currently developing its own antibody tests, although quality concerns have also appeared.
- Prolonged processing times:
Some countries like South Korea have been able to achieve same-day results for COVID-tests, through a combination of easy access to free testing (drive through testing facilities), and having the right infrastructure and processes in place (from lab hardware, stocks of chemicals, logistics, IT and legislation) which the Korean government strengthened after their negative experience dealing with the 2015 MERS outbreak. Meanwhile, other countries in the West are still facing roadblocks that continue to hamper the delivery of results in a timely manner. In the US, where 85% of testing is performed by private labs, average transport time is 24 hours, and average processing time can take another 6 hours. Testing backlogs, like the 80,000 test waitlist at Quest Diagnostics, continue to delay reporting by days. Newer FDA approved tests are showing results in less than 15 minutes, however there are concerns about higher rates of false positives and their scalability given they require samples to be processed one at a time.
- Financial coverage
As countries are beginning to feel the economic impacts of the current pandemic, patients may be disincentivized to get tested if costs prove to be prohibitive. Out-of-pocket costs for COVID-19 tests are covered in the US and in most countries with nationalized healthcare systems, but patients could still potentially be charged for the doctors’ visits and for COVID-related treatment. In India, lack of clarity around who pays for tests has not been fully resolved and have led to delays in production. Efforts are being made to produce low-cost tests for use in developing countries, but low levels of accuracy may hinder their ultimate utilization.
We note that while the $25 billion allocated for testing in the most recent COVID-19 relief package approved by the US Senate could provide the resources needed to help scale up testing more rapidly, decisive action is still needed to ensure adequate testing capacity.
- Challenges implementing contact tracing
From electronic waistbands in Hong Kong to mobile apps in Singapore and QR-code “passports” in mainland China, governments in East Asia have deployed different types of technology to monitor movement, and used information collected from tracing to determine risks of infection spreading within a community. Importantly, tracing was a priority not only for patients tested positive for COVID-19, but also for patients awaiting results and citizens who have traveled internationally and who may be a potential importer of new cases.
For many countries in the West, officials are placing increasing importance on testing and monitoring, but current tracing capacity is still insufficient. In the US, researchers at the federally funded nonprofit Mitre Corp. developed a tool called Sara Alert, which is free for health agencies and lets public health officials enroll and track data on individuals at risk of developing a coronavirus infection. Individuals enter their symptoms into the tool daily, providing public health officials with real-time insights. The US CDC also recently expanded funding for 650 health experts to assist with contact tracing, adding to the current supply of 2,200 tracers currently in the country. By comparison, Wuhan officials required 9,000 tracers to adequately support a population of 11 million. Others have noted that between 100,000 and 300,000 tracers are needed in the US for adequate tracing.
The path forward
As countries and states seek pathways out of lockdown, data and studies are becoming key, following the popular adage “You cannot fight what you cannot see”. Not surprisingly, massive studies using antibody testing are currently underway around the world, from Germany to Italy to New York. In Germany, 3,000 randomly chosen households in Munich (and in other regions) are being asked to allow monthly blood tests for COVID-19 antibodies for a year, with the central aim of understanding how many people – even those who are asymptomatic – have already had the virus. This data, when available, will provide valuable insights in enabling decision-making around how to control the contagion, whilst easing those restrictions that can be safely lifted.
Private sector, governments and foundations are also leveraging AI to understand the pandemic and inform decision making. This effort could prove vital for future potential pandemics. The White House’s COVID-19 Open Research Dataset, which has over 24,000 papers and is constantly being updated, C3.ai and Microsoft’s C3.ai Digital Transformation Institute, and Kaggle’s COVID-19 Open Research Dataset Challenge are examples of this.
Sources
USC and County of Los Angeles Public Health (2020)
Y Analytics aggregates credible findings from leading institutions and researchers. Our goal is to shine a light on the facts made available by content experts and present the implications of these facts. If you have recommendations for additional reputable data sources, insights to help us refine our analysis, or suggested research topics, please contact us at info@yanalytics.org.